Goldman Sachs Explains Everything Traders Need To Know About COVID-19 Vaccines
Tyler Durden
Thu, 10/15/2020 – 17:20
In its latest research note on the subject, Goldman Sachs analysts wrote that their outlook for COVID-19 vaccines receiving their first EUA (emergency approval authorizations) from the FDA in either late December or early January is a key pillar of the firm’s “above consensus” outlook for global growth in 2021. The firm expects growth to peak next summer (between Q2 and Q3) in the US, or next fall (Q3/Q4) in the Euro Area.
Recently, analsyts at the firm have warned that the vaccine outlook is “highly uncertain” and complicated by the issue of public trust, as recent halts to vaccine and therapeutic trials have rattled pubic confidence in the rushed nature of the process.
But assuming the best-case scenario for the vaccine outlook, initial results from Pfizer are expected in October, while Moderna is expected in November. Those “readouts” should show whether the vaccines are effective, or not. Still, with so many people in need of the vaccine, the bank says it believes it willl take “a few quarters” to vaccinate sufficiantly large shares of the population to stop the virus from spreading.
Finally, the firm says it expects vaccines to make the biggest difference in the US and Europe. The impact on EM won’t be as immediately felt, since China has already managed to revive economic growth with substantial state support, while India will likely face a slower rate of acquisition and innoculation, meaning it will likely take longer to rub out the virus.
To offer more clarify, the Goldman team has published a “Q&A” on its vaccine outlook. Read it in full below (text courtesy of Goldman Sachs):
* * *
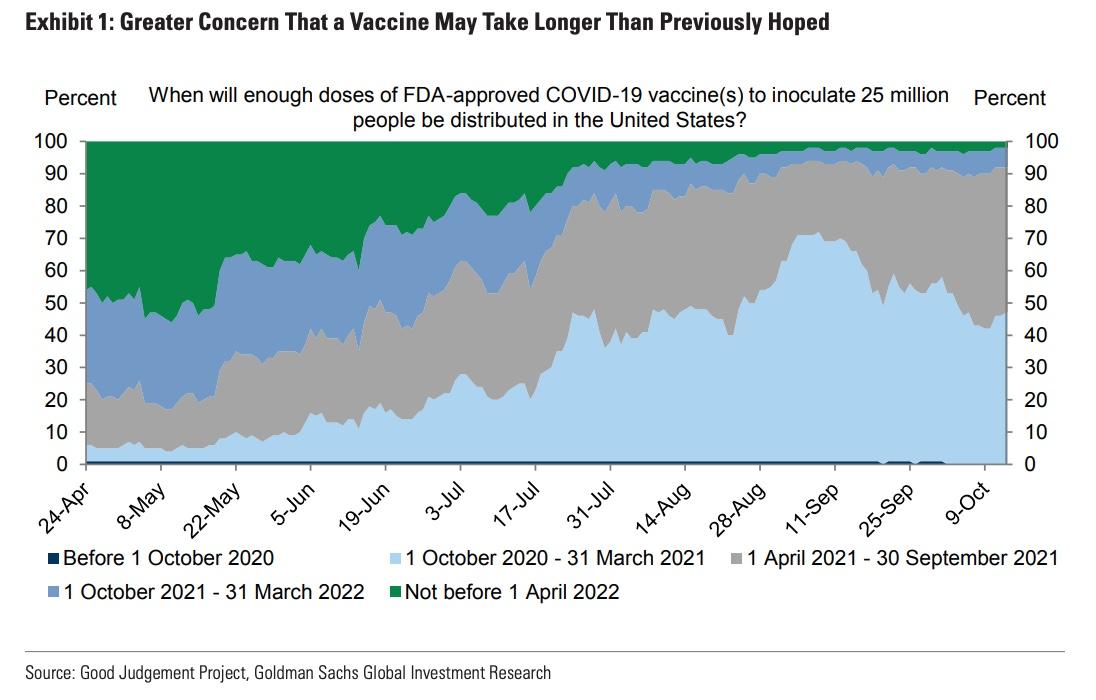
Q: Superforecasters have lowered the odds of inoculating 25mn doses in the US by March to 47%, down from 70% in September. What happened?
A: Declining optimism likely reflects (1) the AstraZeneca trial pause, (2) slower Moderna trial enrollment, and (3) FDA guidelines for emergency approval.
First, the odds started falling with AstraZeneca’s suspension of its trials on September 9 following a second serious spinal inflammatory disorder. While the trial has restarted elsewhere, it is still on hold in the US. Around the same time, the major developers pledged not to rush to market under political pressure. Second, Moderna slowed down trial enrollment to increase participation among Black, Latino and Native American populations, which has now picked up. Third, the FDA issued stricter guidance for approval.
Q: What are the criteria for the FDA to provide Emergency Use Authorization
A: In addition to safety, the key criterion is that the “vaccine efficacy” (VE)—the percent difference of disease between the vaccinated group and unvaccinated control group—is estimated to be at least 50% and that there is sufficient statistical confidence in the VE.2
The EUA guidelines also recommend (1) a median follow-up of at least two months after full vaccination, (2) a submission of a manufacturing plan one month prior, and (3) five or more severe COVID-19 cases in the placebo group.3 While 50% efficacy is necessary for EUA, comments by Peter Marks (FDA) and by Tal Zaks (Moderna) suggest some flexibility on the two months follow-up criterion.4
Q: Pfizer and Moderna have signaled that data readouts are likely to be available by the end of October and in November, respectively. What do successful results look like?
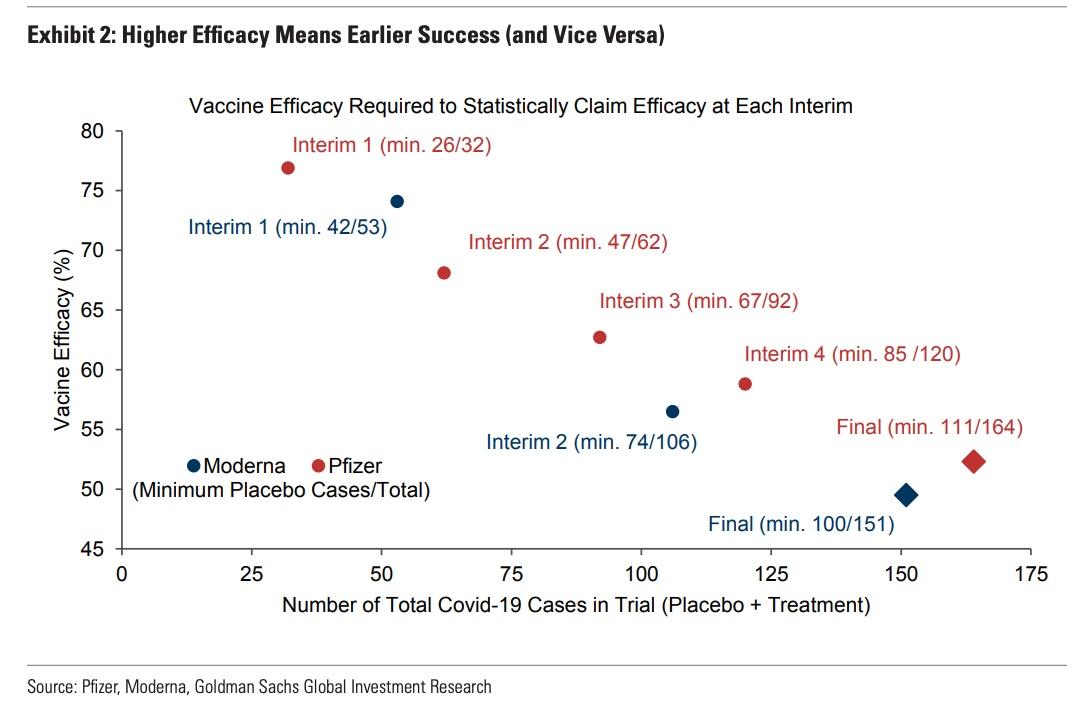
A: While the FDA bar for eventual approval is 50%, vaccine efficacy (VE) rates above 75% would be good news because they would imply high odds of approval by year-end and would bode well for virus control.
Once trials reach a predetermined number of total covid cases, companies can release data readouts. The higher the VE, the earlier (i.e. with fewer total cases) producers will be able to statistically claim VE. For instance, Moderna would have to demonstrate a VE point estimate of at least 75%, implying that at least 42 of the 53 cases occur in the placebo group to claim success in the first interim, whereas for the second interim, Moderna has to pass a point estimate of 57%, and 50% for the final analysis (Exhibit 2). All other things equal, a delay in the data readouts could therefore also send a negative signal about VE.5 A successful readout would also show significant declines in severe diseases, diseases among the elderly, and infections. Crucially, elevated vaccine efficacy would also boost demand and bode well for the ability to (quickly) control the virus.
Q: When do you expect Emergency Use Authorization (EUA) and distribution of the first US dose?
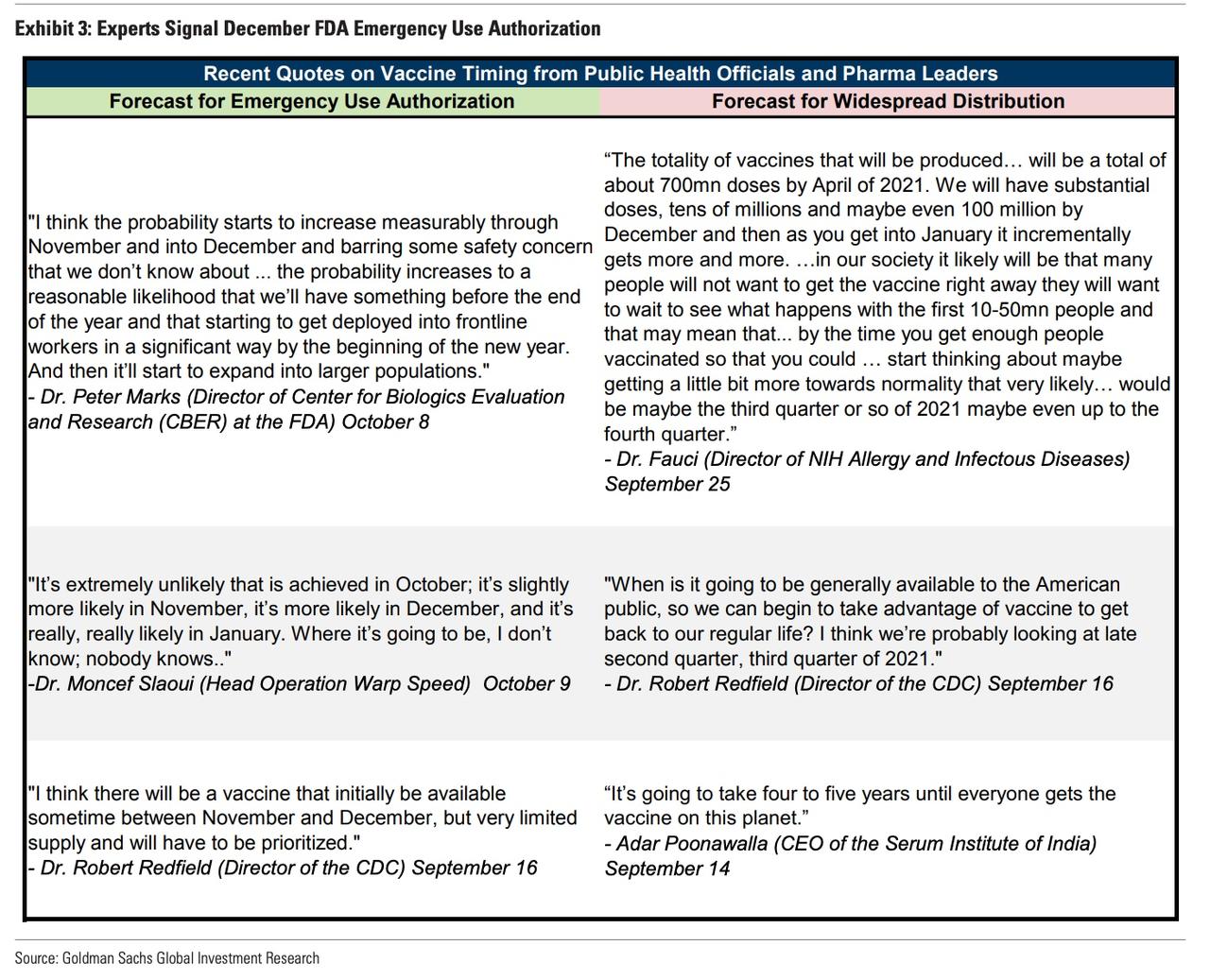
A: Our assumption is that the FDA grants EUA in December, with risks skewed towards January, and that the first dose is inoculated by January
Our assumption of December EUA and a rapid subsequent start to inoculation is consistent with guidance from companies and public health officials (Exhibit 3). Dr. Marks (FDA) expects his staff to analyze data for a “few weeks” and then brief the Advisory Committee meeting, quickly followed by a decision. The risks to the December baseline are skewed towards January, especially if the first interims do not hit the vaccine efficacy- or 5 severe cases criteria.
Q: What is the next approval step after Emergency Use Authorization (EUA)?
A: The FDA expects vaccine producers to prepare a general approval called Biologics License Application (BLA) by finishing the full placebo-controlled trial.
While an EUA requires that a product may be effective and that its benefits outweigh known and potential risks, a BLA requires substantial evidence of safety and effectiveness. While the EUA would likely be processed in a few weeks and plausibly be limited to high risk groups, the BLA would likely take a “few months” to process given the more stringent safety criteria for vaccinating the full population.
Q: Would Europe also relatively rapidly approve a safe and effective vaccine?
A: While we have less visibility on the timeline, that seems quite likely.
The European Medicines Agency (EMA) has an “emergency procedure” which allows for fast-track pandemic approval with an accelerated decision (~70 days vs. 210 days). The EMA also expects the process to be shorter due to the rolling review which has started for AstraZeneca, Pfizer/BioNTech, and likely soon for Moderna too. The UK could issue its own temporary authorization. Successful trials in the US/Europe might also accelerate EMA/FDA approval as agencies can analyze foreign data.
Distribution:
Q: How are countries positioned for success of the leading vaccines?
A: The US would likely benefit from early Pfizer and especially Moderna approvals. AstraZeneca success could quickly benefit multiple regions, including EMs.
The US has sizeable year-end supply commitments with all leading firms. In the EU, approvals of AstraZeneca and Pfizer/BioNTech, both on a rolling review, would especially boost supply. The UK would likely benefit from early approvals of Pfizer/BioNTech and AstraZeneca, given expected year-end doses, while Japan has evenly disbursed contracts, starting in 2021. Many EMs likely depend on AstraZeneca for early widespread access.

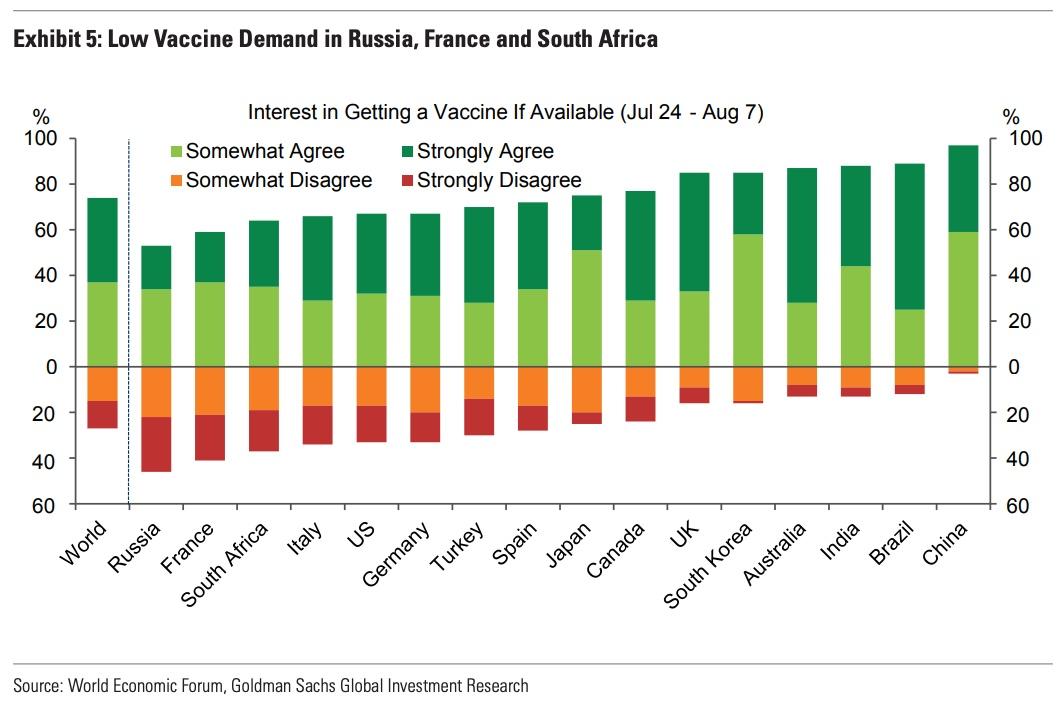
Q: Which countries have the lowest measures of vaccine demand?
A: Globally, a July-August survey shows that 74% of the respondents agree that they would get a vaccine when available (Exhibit 5). In most major economies, reported demand exceeds standard estimates of herd immunity with near universal acceptance in China, Brazil, India and Australia but relatively low levels in Russia, France and South Africa.
Q: What do you make of the decline in some measures of US vaccine confidence?
A: Our base case assumes broad vaccine uptake but this will likely require a safe and very effective vaccine, trust in the approval process, minimal out-of-pocket costs, public campaigns, and time for local evidence and acceptance to build up.
Some measures of US vaccine demand have edged down (Exhibit 6), with slightly less than 40% saying “yes” and 36% currently reporting to be “not sure”. Demand is particularly low in Black, low income and education, and rural communities.7 Four factors are likely weighing on demand:
1. Safety concerns stand out with about 60% of the respondents against getting a vaccine identifying safety/side effects concerns as the key reason.
2. Efficacy concerns around 35% of those against taking a vaccine being concerned. Pew Research Center finds that 55% of respondents would reconsider their decision to take the vaccine if it was only 60% effective.
3. Politicization has likely played a role too with less than half of Americans thinking the FDA should fast-track approval.
4. Out-of-pocket costs worry US respondents. While the CARES Act requires health insurers to cover the vaccine after full FDA approval, it doesn’t require coverage under EUA. The Biden/Harris campaign has pledged to distribute vaccines at no cost, in line with the National Academy of Medicine recommendation.

Q: Who will get the vaccines first?
In the US, the National Academy of Medicine (NAM) plan defines three prioritized phases in order of fatality, infection, and transmission risk, while also focusing on important societal functions (Exhibit 7, left panel).

The UK plans to distribute primarily by age starting with the elderly, while EU countries have their own frameworks. Most nations, including China, have subscribed to the WHO’s COVAX Plan, which pledges to evenly distribute pooled vaccines for healthcare and social care workers first (up to 3% of the population) and then for the elderly (>65) and people with comorbidities (up to 20% of the population).
While highly uncertain and contingent on take-up, tiered distribution of a safe and effective vaccine should lead to front-loaded public health benefits, starting in Q1 in the US.
Q: When do you expect widespread US vaccination to start?
A: We expect Phase 2, targeting 105mn people in moderate risk and high impact professions, to start in March.
We expect inoculation to begin in the US in January with an estimated 50-80mn doses of supply by year-end.10 The initial supply and ongoing production will likely quickly cover Phase 1 of healthcare workers and very high risk populations. Given potential supply chain hiccups, startup costs in the distribution, and the CDC’s goal to maximize vaccine acceptance with the initial doses, we assume that the Phase 2 will not start until March, from which point onward vaccine supply could exceed demand. US vaccine adoption will then likely ramp up in line with demand through Q2 until reaching widespread levels sometime later in 2021 according to Dr. Fauci (NIH) and Dr. Redfield (CDC), as shown in Exhibit 3.
Q: When will widespread vaccination start in Europe?
A: Probably in early Q2 in the UK and late Q2 in the EU. That is bit later than in the US due to lower visibility on the approval timeline and less front-loaded EU supply contracts.
Front-loaded supply contracts position the UK well to start distribution in Q1 and distribute widely in early Q2, shortly after the US (even if public health officials appear more focused on vulnerable groups than rapid widespread adoption). Germany, France, Italy and the Netherlands could begin soon after the UK with large national supply contracts, which allowed Germany and France to opt out of Covax. Elsewhere in Europe, widespread distribution might not begin until early Q3 due to the potential dependence on EU supply contracts, distributed based on population, and Covax.
Q: What about widespread vaccination in EMs?
A: While targeted vaccination has already started in China and Russia, the EM vaccination outlook is more uncertain, very heterogeneous, and less positive, on net, than in DMs.
On the positive side, vaccination has already begun in Russia and China. Russia’s Gamaleya’s Sputnik V vaccine is approved for vulnerable populations with broader usage announced for January. China has approved three vaccines for emergency civilian use (two from the China National Biotec Group and one from Sinovac) and the CanSino vaccine for the military. While the absence of Phase 3 results creates uncertainty, the decision to rapidly vaccinate “hundreds of thousands” of people with relatively low virus circulation suggests officials might be confident in the vaccines. It is also plausible that a nonnegligible fraction of the population in several EMs such as India and Brazil may already have been infected by early next year and would therefore not need a vaccine assuming protection lasts. Additionally, the much lower hospitalization and fatality rates among young individuals and their larger population share may also help EM policymakers to manage scarcity by targeting the elderly.
On the negative side, the available EM advance purchases are generally much smaller than in DMs, especially on a per capita basis, despite support from COVAX and CEPI. Currently, COVAX has commitments that amount to 500mn doses and targets 1000mn doses. Overall, vaccine adoption will likely lag significantly behind in several lower income economies with Adar Poonwalla (Serum Institute of India) not expecting widespread global vaccination until four-five years from now. Seasonal or annual shots rather than a multi-year or lifelong vaccine due to potentially short-lived protection could also pose challenges to EMs with poor health infrastructure.
Growth effects:
Q: Achieving virus control and normalization with a vaccine likely requires elevated vaccine efficacy (VE) and elevated demand.12 Which of the two factors poses the largest downside risk?
A: While both are highly uncertain, we see the largest downside risk from demand.
Experts such as Dr. Krammer and Dr. Saville are constructive on the outlook for vaccine efficacy, reflecting (1) evidence of protection in animal studies, (2) the level of neutralizing antibodies, and (3) few natural reinfections (so far).13 Experts including Dr. Fauci are more concerned about vaccine demand (Exhibit 3). Demand concerns reflect limited vaccine confidence (Exhibit 6) and the risk it erodes further with insufficient efficacy, “expected” adverse reactions (e.g. fever), short-lived protection, or misattribution of unrelated negative health outcomes to the vaccine.
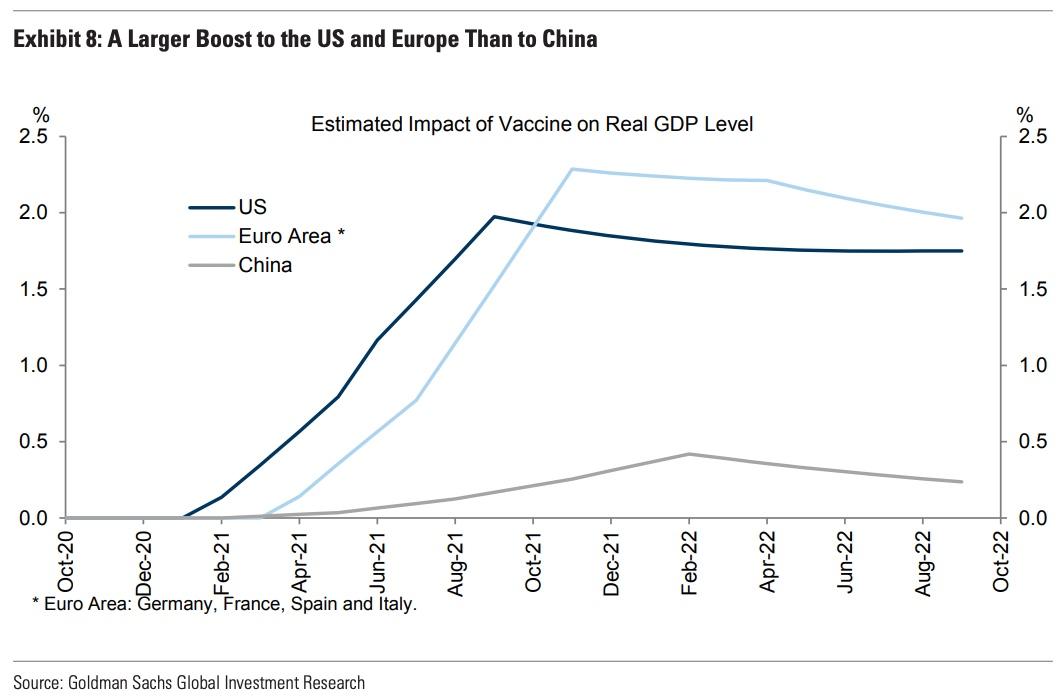
Q: How large will the vaccine boost to GDP be?
A: We expect the vaccine to boost the end-2021 level of US and Euro Area GDP by around 2%, with the largest boost to growth in Q2-Q3 in the US and Q3-Q4 in the Euro Area.
Exhibit 8 updates our model of the growth effects of a vaccine through a more complete recovery in high-contact industries such as restaurants and travel and through more limited scarring effects.
The simulations generate three results. First, we estimate that the vaccine boosts the end-2021 level of GDP by around 2% both in the US and the Euro Area. The US boost is somewhat less large than estimated previously, mostly because of the faster-than-expected recovery. Second, under our timing assumptions for widespread distribution, the largest growth boost occurs in Q2-Q3 in the US and Q3-Q4 in the Euro Area.14 The boost is somewhat gradual because potentially later broad-use approval and measures of vaccine confidence suggest that distributing to sufficiently large shares of the population will likely take a few quarters. Third, the China boost is much smaller because virus control and activity are already solid.
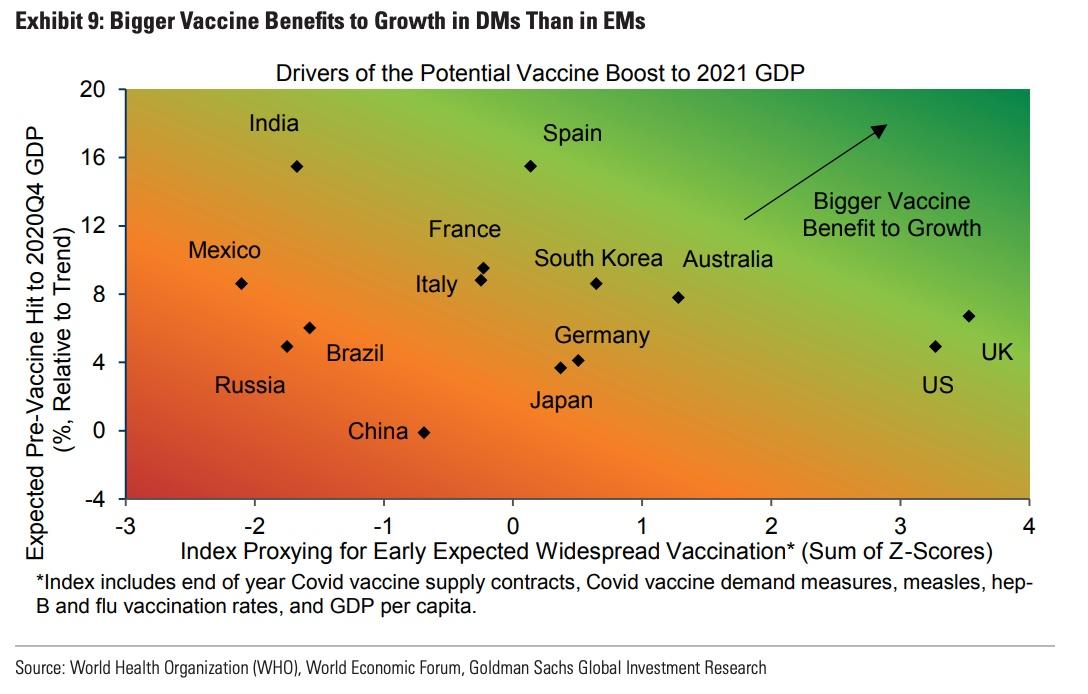
Q: More broadly, which countries are likely to see the largest vaccine boost to GDP?
A: We expect a larger vaccine boost to 2021 growth in DMs such as the US, the UK, and Spain than in EMs such as India and China.
We qualitatively extend the insights from our model to more countries. The vaccine GDP boost rises with (1) an earlier and more widespread vaccination and (2) a larger virus GDP hit without a vaccine. Exhibit 9 plots (1) a vaccination index on the horizontal axis (using data on year-end supply contracts, a demand index using covid-19 vaccine surveys and actual vaccination rates, and GDP per capita) and (2) the expected virus hit to 2020Q4 GDP on the vertical axis.15 The upshot is that the vaccine boost to 2021 growth should be larger in DMs such as the US and the UK (strong placement for early widespread vaccination) and Spain (large virus GDP hit) than in EMs such as India and Mexico (slower vaccine acquisition and distribution) and China (output already close to normal).
* * *
Source: Goldman Sachs
![]()
Zero Hedge’s mission is to widen the scope of financial, economic and political information available to the professional investing public, to skeptically examine and, where necessary, attack the flaccid institution that financial journalism has become, to liberate oppressed knowledge, to provide analysis uninhibited by political constraint and to facilitate information’s unending quest for freedom. Visit https://www.zerohedge.com