
“Pandemic is Over” – Former Pfizer Chief Science Officer Says “Second Wave” Faked On False-Positive COVID Tests
Tyler Durden
Sun, 11/22/2020 – 23:00
This video provides one of the most erudite and informative looks at Covid-19 and the consequences of lockdowns. As AIER notes, it was remarkable this week to watch as it appeared on YouTube and was forcibly taken down only 2 hours after posting.
The copy below is hosted on LBRY, a blockchain video application. In a year of fantastic educational content, this is one of the best we’ve seen.

Consider the presenter’s bio:
Dr. Michael Yeadon is an Allergy & Respiratory Therapeutic Area expert with 23 years in the pharmaceutical industry. He trained as a biochemist and pharmacologist, obtaining his PhD from the University of Surrey (UK) in 1988.
Dr. Yeadon then worked at the Wellcome Research Labs with Salvador Moncada with a research focus on airway hyper-responsiveness and effects of pollutants including ozone and working in drug discovery of 5-LO, COX, PAF, NO and lung inflammation. With colleagues, he was the first to detect exhaled NO in animals and later to induce NOS in lung via allergic triggers.
Joining Pfizer in 1995, he was responsible for the growth and portfolio delivery of the Allergy & Respiratory pipeline within the company. He was responsible for target selection and the progress into humans of new molecules, leading teams of up to 200 staff across all disciplines and won an Achievement Award for productivity in 2008.
Under his leadership the research unit invented oral and inhaled NCEs which delivered multiple positive clinical proofs of concept in asthma, allergic rhinitis and COPD. He led productive collaborations such as with Rigel Pharmaceuticals (SYK inhibitors) and was involved in the licensing of Spiriva and acquisition of the Meridica (inhaler device) company.
Dr. Yeadon has published over 40 original research articles and now consults and partners with a number of biotechnology companies. Before working with Apellis, Dr. Yeadon was VP and Chief Scientific Officer (Allergy & Respiratory Research) with Pfizer.
What likely triggered the Silicon Valley censor-mongers is the fact that a former Chief Science Officer for the pharmaceutical giant Pfizer says “there is no science to suggest a second wave should happen.” The “Big Pharma” insider asserts that false positive results from inherently unreliable COVID tests are being used to manufacture a “second wave” based on “new cases.”
As Ralph Lopez write at HubPages, Yeadon warns that half or even “almost all” of tests for COVID are false positives. Dr. Yeadon also argues that the threshold for herd immunity may be much lower than previously thought, and may have been reached in many countries already.
In an interview last week (see below) Dr. Yeadon was asked:
“we are basing a government policy, an economic policy, a civil liberties policy, in terms of limiting people to six people in a meeting…all based on, what may well be, completely fake data on this coronavirus?”
Dr. Yeadon answered with a simple “yes.”
Even more significantly, even if all positives were to be correct, Dr. Yeadon said that given the “shape” of all important indicators in a worldwide pandemic, such as hospitalizations, ICU utilization, and deaths, “the pandemic is fundamentally over.”
Yeadon said in the interview:
“Were it not for the test data that you get from the TV all the time, you would rightly conclude that the pandemic was over, as nothing much has happened. Of course people go to the hospital, moving into the autumn flu season…but there is no science to suggest a second wave should happen.”
In a paper published this month, which was co-authored by Yeadon and two of his colleagues, “How Likely is a Second Wave?”, the scientists write:
“It has widely been observed that in all heavily infected countries in Europe and several of the US states likewise, that the shape of the daily deaths vs. time curves is similar to ours in the UK. Many of these curves are not just similar, but almost super imposable.“
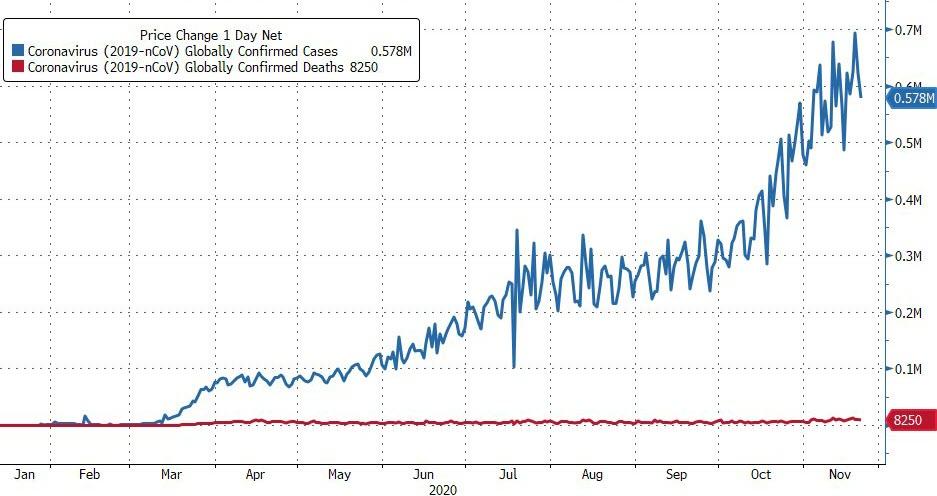
In the data for UK, Sweden, the US, and the world, it can be seen that in all cases, deaths were on the rise in March through mid or late April, then began tapering off in a smooth slope which flattened around the end of June and continues to today. The case rates however, based on testing, rise and swing upwards and downwards wildly.
Media messaging in the US is already ramping up expectations of a “second wave.”
The survival rate of COVID-19 has been upgraded since May to 99.8% of infections. This comes close to ordinary flu, the survival rate of which is 99.9%. Although COVID can have serious after-effects, so can flu or any respiratory illness. The present survival rate is far higher than initial grim guesses in March and April, cited by Dr. Anthony Fauci, of 94%, or 20 to 30 times deadlier. The Infection Fatality Rate (IFR) value accepted by Yeadon et al in the paper is .26%. The survival rate of a disease is 100% minus the IFR.
Dr. Yeadon pointed out that the “novel” COVID-19 contagion is novel only in the sense that it is a new type of coronavirus. But, he said, there are presently four strains which circulate freely throughout the population, most often linked to the common cold.
In the scientific paper, Yeadon et al write:
“There are at least four well characterised family members (229E, NL63, OC43 and HKU1) which are endemic and cause some of the common colds we experience, especially in winter. They all have striking sequence similarity to the new coronavirus.”
The scientists argue that much of the population already has, if not antibodies to COVID, some level of “T-cell” immunity from exposure to other related coronaviruses, which have been circulating long before COVID-19.
The scientists write:
“A major component our immune systems is the group of white blood cells called T-cells whose job it is to memorise a short piece of whatever virus we were infected with so the right cell types can multiply rapidly and protect us if we get a related infection. Responses to COVID-19 have been shown in dozens of blood samples taken from donors before the new virus arrived.”
Introducing the idea that some prior immunity to COVID-19 already existed, the authors of “How Likely is a Second Wave?” write:
“It is now established that at least 30% of our population already had immunological recognition of this new virus, before it even arrived…COVID-19 is new, but coronaviruses are not.”
They go on to say that, because of this prior resistance, only 15-25% of a population being infected may be sufficient to reach herd immunity:
“…epidemiological studies show that, with the extent of prior immunity that we can now reasonably assume to be the case, only 15-25% of the population being infected is sufficient to bring the spread of the virus to a halt…”
In the US, accepting a death toll of 200,000, and a survival rate of 99.8%, this would mean for every person who has died, there would be about 400 people who had been infected, and lived. This would translate to around 80 million Americans, or 27% of the population. This touches Yeadon’s and his colleagues’ threshold for herd immunity.
Finally, the former Pfizer executive and scientist singles out one former colleague for withering rebuke for his role in the pandemic, Professor Neil Ferguson. Ferguson taught at Imperial College while Yeadon was affiliated. Ferguson’s computer model provided the rationale for governments to launch draconian orders which turned free societies into virtual prisons overnight. Over what is now estimated by the CDC to be a 99.8% survival rate virus.
Dr. Yeadon said in the interview that “no serious scientist gives any validity” to Ferguson’s model.
Speaking with thinly-veiled contempt for Ferguson, Dr. Yeadon took special pains to point out to his interviewer:
“It’s important that you know most scientists don’t accept that it [Ferguson’s model] was even faintly right…but the government is still wedded to the model.”
Yeadon joins other scientists in castigating governments for following Ferguson’s model, the assumptions of which all worldwide lockdowns are based on. One of these scientists is Dr. Johan Giesecke, former chief scientist for the European Center for Disease Control and Prevention, who called Ferguson’s model “the most influential scientific paper” in memory, and also “one of the most wrong.”
It was Ferguson’s model which held that “mitigation” measures were necessary, i.e. social distancing and business closures, in order to prevent, for example, over 2.2 million people dying from COVID in the US.
Ferguson predicted that Sweden would pay a terrible price for no lockdown, with 40,000 COVID deaths by May 1, and 100,000 by June. Sweden’s death count is under 6,000. The Swedish government says this coincides to a mild flu season. Although initially higher, Sweden now has a lower death rate per-capita than the US, which it achieved without the terrific economic damage still ongoing in the US. Sweden never closed restaurants, bars, sports, most schools, or movie theaters. The government never ordered people to wear masks.

Dr. Yeadon speaks bitterly of the lives lost as a result of lockdown policies, and of the “savable” countless lives which will be further lost, from important surgeries and other healthcare deferred, should lockdowns be reimposed.
Watch the full discussion below:
Yeadon’s warnings are confirmed by a new study from the Infectious Diseases Society of America., summarized succinctly in the following twitter thread from al gato malo (@boriquagato)
Anyone still presuming that a Positive PCR test is showing a COVID case needs to read this very carefully:
-
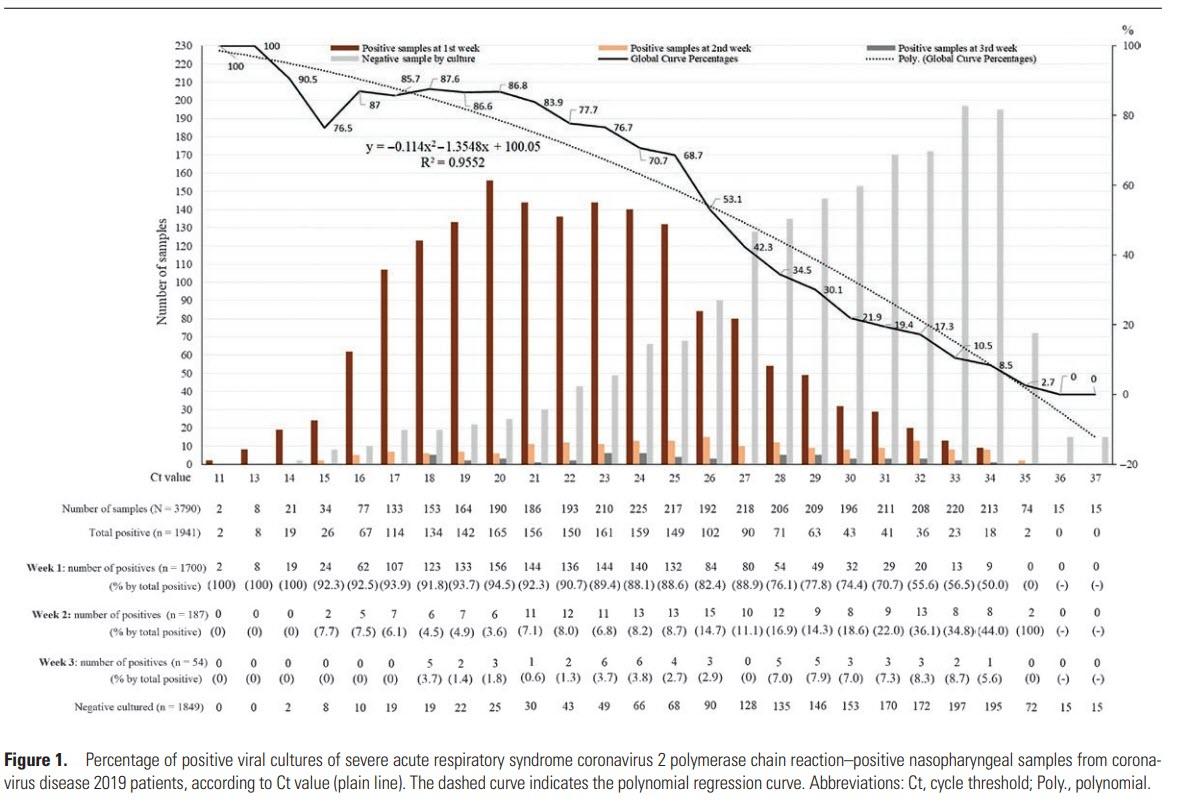
even 25 cycles of amplification, 70% of “positives” are not “cases.” virus cannot be cultured. it’s dead.
-
by 35: 97% non-clinical.
-
the US runs at 40, 32X the amplification of 35.
a lot of people still seem to not understand what this means, so let’s lay that out for a minute.
PCR tests look for RNA. there is too little in your swab. so they amplify it using a primer based heating and annealing process.
Each cycle of this process doubles the material
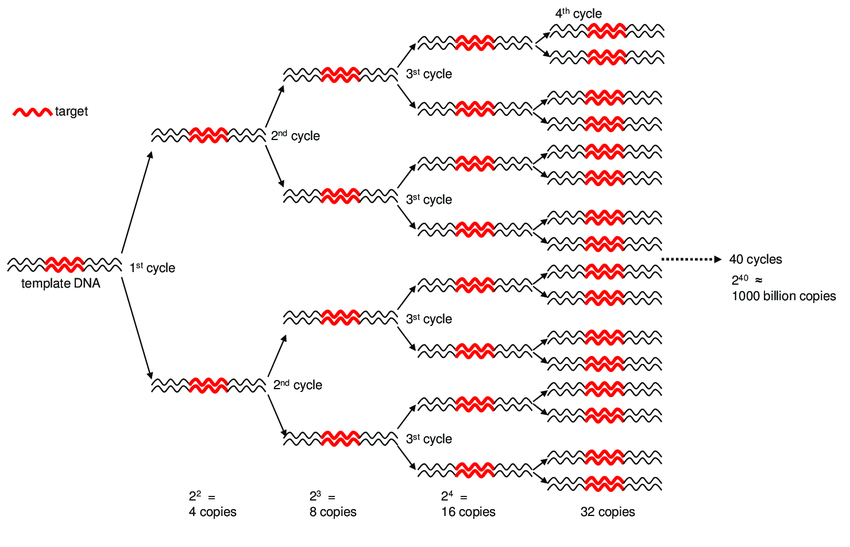
the US (and much of the world) is using a 40 Ct (cycle threshold). so, 40 doublings, 1 trillion X amplification.
This is absurdly high.
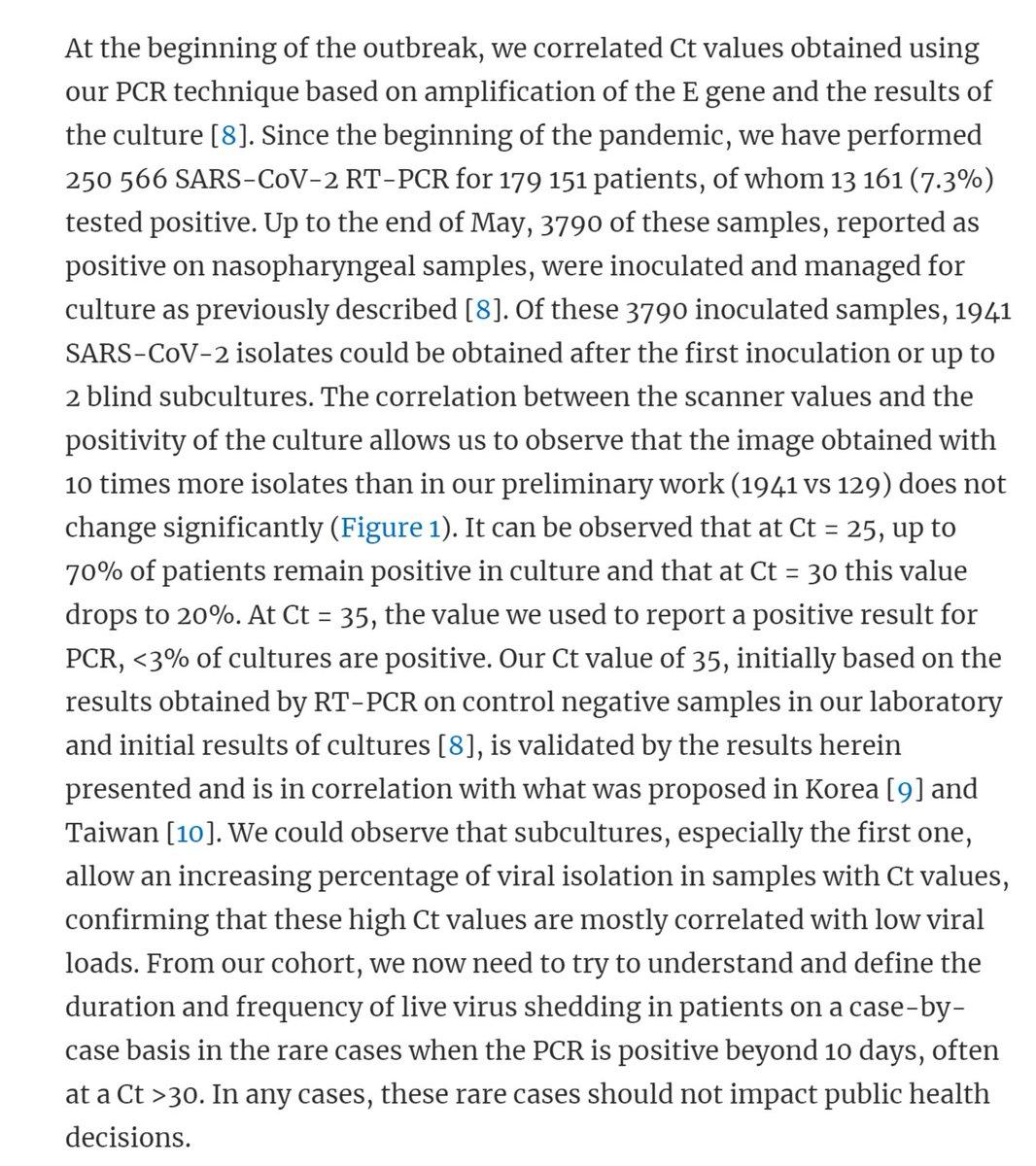
The way that we know this is by running this test, seeing the Ct to find the RNA, and then using the same sample to try to culture virus.
If you cannot culture the virus, then the virus is “dead.” it’s inert. if it cannot replicate, it cannot infect you or others. it’s just traces of virus, remnants, fragments etc
PCR is not testing for disease, it’s testing for a specific RNA pattern and this is the key pivot
When you crank it up to 25, 70% of the positive results are not really “positives” in any clinical sense.
i hesitate to call it a “false positive” because it’s really not. it did find RNA.
but that RNA is not clinically relevant.
It cannot make you or anyone else sick
so let’s call this a non-clinical positive (NCP).
-
if 70% of positives are NCP’s at 25, imagine what 40 looks like. 35 is 1000X as sensitive.
-
this study found only 3% live at 35
-
40 Ct is 32X 35, 32,000X 25
no one can culture live virus past about 34 and we have known this since march. yet no one has adjusted these tests.
presuming it bears out, this is a key finding.
it shows that many patients that are PCR+ for COV-19 are not shedding infectious virus.
this would imply shorter quarantine needed and provide a testable basis for discharge of isolated patients. pic.twitter.com/UvumjkxVxv
— el gato malo (@boriquagato) March 27, 2020
This is more very strong data refuting the idea that you can trust a PCR+ as a clinical indicator.
That is NOT what it’s meant for. at all.
Using them to do real time epidemiology is absurd.
The FDA would never do it, the drug companies doing vaccine trials would never do it… it’s because it’s nonsense.
And this same test is used for “hospitalizations” and “death with covid” (itself a weirdly over inclusive metric)
PCR testing is not the answer, it’s the problem.
It’s not how to get control of an epidemic, it’s how to completely lose control of your data picture and wind up with gibberish and we have done this to ourselves before.
The last major false positive pseudo-epidemic was Swine Flu in 2009. Everyone said we would never let it happen again. pic.twitter.com/Hdif5l5Gam
— Dr Clare Craig (@ClareCraigPath) November 16, 2020
A quick word what this data does and does not mean.
Saying “a sample requiring 35 Ct to test + has a 3% real clinical positive rate” does not mean “97% of + tests run at 35 Ct are NCP’s”
People seem to get confused on this, so lets explain:
Most tests are just amplified and run. they don’t test every cycle as these academics do. that would make the test slow and expensive, so you just run 40 cycles then test.
Obviously, a real clinical positive (RCP) that would have been + at 20 is still + at 40.
but when you run the tests each cycle as the academics do, that test would already have dropped out.
so saying that only 3% at 35 are RCP really means that 3% of those samples not PCR + at 34 were PCR and RCP + at 35.
this lets us infer little about overall NCP/RCP rate.
so we cannot say “at 25 Ct, we have a 70 NCP rate.” in fact, it’s hard to say much of anything. it depends entirely on what the source material coming in looks like.
you cannot even compare like to like.
This is what i mean by “the data is gibberish”
Today at 40 Ct, 7% PCR positive rate could be 1% RCP prevalence when that same thing meant 6% RCP prev in april.
If there is lots more trace virus around, more people who have recovered and have fragments left over, etc this test could be finding virus you killed 4 months ago.
So if we consider RCP rate/PCR+ rate, we would expect that number to drop sharply late in an epidemic because there is more dead virus around for PCR to find, but we have no idea what that ratio is or how it changes.
This spills over in to deaths, reported hospitalization etc.
Testing is being made out to be like the high beams on a car, but when it’s snowing like hell at night, that is the LAST thing you want. It is not illuminating our way, it’s blinding us.
A bad inaccurate map is much worse than no map at all, and this is a world class bad map…
We’re basing policy that is affecting billions of humans on data that is uninterpretable gibberish.
It’s a deranged technocrat’s wet dream, but for those of us along for the ride, it’s a nightmare.
Testing is not the solution, it’s the problem.
Any technocrat or scientist that does not know this by now is either unfit for their job or has decided that they just don’t care and prefer power to morality.
This is, of curse, precisely the kind of person who winds up running a gov’t agency… oopsie.
The head of the NIH is not the best scientist, it’s the best politician.
All this wild and reckless government policy has never been about the science.
It’s politics and panic.
You can read the whole paper here:
![]()
Zero Hedge’s mission is to widen the scope of financial, economic and political information available to the professional investing public, to skeptically examine and, where necessary, attack the flaccid institution that financial journalism has become, to liberate oppressed knowledge, to provide analysis uninhibited by political constraint and to facilitate information’s unending quest for freedom. Visit https://www.zerohedge.com