
The Decimal Point That Blew Up The World
Tyler Durden
Thu, 12/17/2020 – 19:20
Authored by Jeffrey Tucker via The American Institute for Economic Research,
What was the basis of panic that led the lights to darken on civilization?
The most important date here might be March 11, 2020. That’s when Congress itself flew into an unwarranted panic, and acquiesced to a lockdown at the urging of the “experts.”
State governors followed one by one, with few exceptions, and the rest of the world joined the lockdown frenzy.

In February, people were aching to know the answer to the following.
Would this “novel virus” have familiar patterns we associate with the flu, seasonal colds, and other predictable and manageable pathogens? Or would this be something entirely different, unprecedented in our lifetimes, terrifying, and universally deadly?
Crucial in this stage was public-health messaging. In previous pandemics from post-1918 throughout the 20th century, the central messaging was to stay calm, go to the doctor if you feel sick, avoid deliberately infecting others, and otherwise trust the systems in place and keep society functioning. This was long considered responsible public-health messaging, and this was pretty much where we stood throughout most of January and February, when publications regardless of their political outlook maintained sobriety and rationality.
Something dramatically changed this time. They pushed panic, tapping into a primal fear of disease. The reality of pandemic, as it turns out, has been familiar. The severity of its impact has been radically disparate across demographics, hitting mainly the elderly and infirm with 40% of deaths tracing to long-term care facilities with an average age of death nearly equal to the average lifespan. It is regionally migratory. It follows a seasonal pattern from pandemic to its endemic equilibrium.
What has been different has been the messaging that has almost universally been structured to create public frenzy, from the New York Times’s February 28 urge to “go medieval” to Salon’s latest demand that we panic even more.
My own sense of impending doom began on March 6 with the cancellation of South by Southwest in Austin, Texas, an action of the mayor alone, and completely without modern precedent. I wrote about it on March 8. Four days later, President Trump gave a nationwide address that ended with a shocking announcement that all flights from Europe would be stopped to keep the coronavirus out even though the virus had been here since January. The next day, on March 13, the administration issued what amounted to a shutdown plan for the nation.
This timeline, however, misses a crucial step.
We should be grateful to Ronald B. Brown of Waterloo University for his extraordinary paper that appears in Disaster Medicine and Public Health Preparedness (Vol 14, No. 3): “Public Health Lessons Learned From Biases in Coronavirus Mortality Overestimation.” It also appears on the website of the National Institutes of Health with a date of August 12.
Our author’s thesis was that the wild overreaction and unprecedented lockdowns of life began with what was a terminological mixup that led to a misplacement of a decimal point in a report from the National Institutes of Health.
It was a seemingly small error but it provided the basis on which Anthony Fauci testified at the House Oversight and Reform Committee about the seriousness of novel coronavirus spreading across the globe.
Here is the video in question. As you watch, you will note the seeming precision of data that actually masks a huge problem. He obscures the huge difference between the infection fatality rate, the case fatality rate, and the overall death rate. Nowhere does he mention survival rates. Not one person present pushed back on his claims. In the blizzard of data, he finally summarizes in a way that terrified everyone. Covid, he said, is “10 times more lethal than the seasonal flu.”
Even apart from that prediction, his entire demeanor was: this is entirely new, very deadly, and unbearably unmanageable without extreme measures. Fauci’s implicit message to Congress and the American people was that it is time to panic.
Fauci was claiming what in fact he could not know, conflating two distinct data sets, and extrapolating in ways that allowed him to make a completely unsupported claim that very obviously turned out to be false. Two years ago, 61,000 Americans of all ages died of flu, exclusive of other ailments.
If you incorrectly impose on that a “case fatality rate” of 0.1% and extrapolate to Covid infections, you end up with at least 800,000 deaths from Covid alone – not “with” or “involving” Covid as the CDC classifies deaths today (that alone represents a big change). This is a scary prediction at the time; it seemed to add weight to the estimates out of the Imperial College of London that 2.2 million people would die without locking down. This testimony led a whole generation of lawmakers to believe that none of the traditional medical measures could or would work. There is no comparing this with the flu or any respiratory illness. This was the Other that justified a once-in-many-generations national emergency that required an end to our way of life.
The trouble is that the whole claim was based on a terminological misstatement that fed a basic math error. As Brown explains:
Sampling bias in coronavirus mortality calculations led to a 10-fold increased mortality overestimation in March 11, 2020, US Congressional testimony. This bias most likely followed from information bias due to misclassifying a seasonal influenza IFR as a CFR, evident in a NEJM.org editorial. Evidence from the WHO confirmed that the approximate CFR of the coronavirus is generally no higher than that of seasonal influenza. By early May 2020, mortality levels from COVID-19 were considerably below predicted overestimations, a result that the public attributed to successful mitigating measures to contain the spread of the novel coronavirus.
Let’s follow Brown here as he takes the reader through the crucial differences between the IFR and the CFR. IFRs from samples across the population “include undiagnosed, asymptomatic, and mild infections.” To calculate the average IFR across the population, you do randomized samples to judge its prevalence. The results are inclusive of cases – what we used to call actual “sick” people – but extend to people who merely carry traces of the dead virus but are in no substantial danger of passing it onward or experiencing any severe outcomes. Cases, on the other hand, “are based exclusively on relatively smaller groups of moderately to severely ill diagnosed cases at the beginning of an outbreak.” The CFR is a smaller group. Brown provides the following graphic to show how epidemiology has long considered the difference.

Based on this graphic alone, you can see why it becomes crucial to keep these terms straight.
The CFR is higher; IFR is lower; the crude mortality rate is lower still.
The CFR measures severity; the IFR measures prevalence.
Those are the two general issues one needs to know to assess whether and to what extent a virus outbreak is mild, moderate, serious, or severe. This matters due to the long-observed evolved reality of respiratory viruses: there is a trade off between the forces. The more severe the virus, the quicker it burns itself out. The milder (and “smarter”) it is, the more it can spread. To mix up severity and prevalence is to make a mess of all the important categories that infectious disease specialists use to assess the social impact of a new virus.
Moreover, if you are going to compare how severe a pandemic is, you have to compare apples to apples, which means at the very minimum that we must be careful to distinguish apples from oranges from pears. That is precisely what the early messaging surrounding the coronavirus did not do.
Cases are not deaths; even more crucially, cases in a traditional sense mean that people are actually sick, not merely that they have been tested positive by a PCR test. Adding to the confusion, most data sources on Covid today use the term “cases” to identify any positive test, with or without symptoms, when the correct word would be “infections.” Further, the PCR test itself presents its own problems. As Brown notes, “A serious limitation of RT-PCR testing is that nucleic acid detection is not capable of determining the difference between infective and noninfective viruses.” The widespread use of the PCR test has made its own contribution to blurring all these crucial distinctions.
Now consider an extraordinary article from the New England Journal of Medicine that appeared on February 28, with Anthony Fauci as the co-author. The import of the piece was to claim that Covid and flu are quite similar in severity.
“The overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
What matters here is not the prediction as such but the switching of the word infection with case: the flu has “a case fatality rate of approximately 0.1%.” This was incorrect even at the time of writing. You can call it a misprint or sloppy or downright duplicitous. Regardless, even the World Health Organization had identified the 0.1% figure as the flu’s infection fatality rate. If you assume one symptomatic confirmed case for every infection (or what is now confusingly called “cumulative cases”), the error could be a misplace decimal: 0.01% not 0.1%. Regardless, Fauci’s article directly contradicted the WHO, and ran counter to everything that was already then known. But his CFR claim about flu is precisely what led him to claim in front of the Congressional committee that Covid would be deadly in ways that defy all experience of this generation.
Brown further explains:
As the campaign to mitigate coronavirus transmission was implemented from March into May, 2020, expected coronavirus mortality totals in the United States appeared much lower than the overestimation reported in Congressional testimony on March 11. Compared with the most recent season of severe influenza A (H3N2) in 2017-2018,with 80,000 US deaths reported by CDC officials, US coronavirus mortality totals had just reached 80,000 on May 9, 2020. By then, relative to the 2017-2018 influenza, it was clear that the coronavirus mortality total for the season would be nowhere near 800,000 deaths inferred from the 10-fold mortality overestimation reported to Congress. Even after adjusting for the effect of successful mitigation measures that may have slowed down the rate of coronavirus transmission, it seems unlikely that so many deaths were completely eliminated by a nonpharmaceutical intervention such as social distancing, which was only intended to contain infection transmission, not suppress infections and related fatalities. Also in early May, 2020, a New York State survey of 1,269 COVID-19 patients recently admitted to 113 hospitals found that most of the patients had been following shelter-in-place orders for 6 wk, which raised state officials’ suspicions about social distancing effectiveness. Still, polls showed the public credited social distancing and other mitigation measures for reducing predicted COVID-19 deaths, and for keeping people safe from the coronavirus.
As of this writing, however, deaths “involving” or “with” Covid has passed 300,000, which while less than half as high as what Congress heard they would be on March 11, is still quite high, provided these deaths have not been broadly misclassified. However, on March 24, the CDC made an announcement of serious significance. It would now calculate coronavirus mortality by including “probable” and “likely” deaths in the International Classification of Diseases code (ICD).
This became an invitation to misclassification. People who otherwise would have previously been classified as having heart disease or some other comorbidity could now be classified as Covid. This also included a financial incentive to do just that. For this reason, when the CDC announced that “for 6% of the deaths, Covid-19 was the only cause mentioned,” it came as a shock to people. What that means is that 94% of the deaths attributed to Covid were associated with additional comorbidities that prevented the immune system from fighting off the virus.
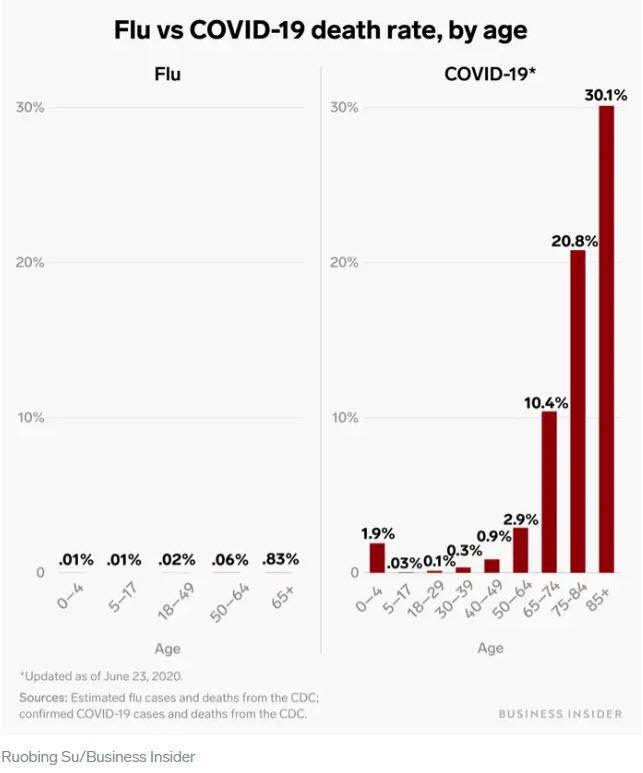
Following the March 11 Fauci testimony, in which he conflated IFR and CFR, the national media went wild with Covid and flu comparison. The following article, for example, blew up from BusinessInsider in June: “The coronavirus death rate in the US is almost 50 times higher than that of the flu. See how they compare by age bracket.” If you look carefully at the charts, you can see something fishy: they calculated infection fatality rate for flu against the case fatality rate for Covid. That necessarily generates a wild overestimate for Covid deaths. The charts are terrifying – and have nothing to do with reality.
Let’s hop forward from the testimony days to one month later when full-scale panic had already hit the U.S. Speaking at a White House press conference, Fauci then made a claim that strains credulity at every level. He said at a White House press briefing that the stringencies and “social distancing” could not and would not be relaxed until there are no “no new cases, no deaths.” Such a thing has happened only once in the history of viruses: smallpox. From the first experiments with inoculation to the final eradication took some 250 years. And yet here we have Fauci explaining that life could not be normal and functioning again until this widespread virus, relatively mild for 95% of the population, was completely eradicated from the planet!
And now we have the vaccine, and plenty of questions remaining about it, such as why non-vulnerable populations would prefer to take it over gaining the exposure necessary for naturally acquired immunity. Asking such a basic question is very close to being tabooed, even as lawmakers and other institutions are toying with the idea of making it mandatory. Even then, many of the lockdown advocates from earlier this year are saying that it will not enable us to go back to normal, to take off the masks, to go to the movies, or travel again. This is precisely the belief you might expect from a crowd that participated in what John Iaonnidis called a “one-in-a-century evidence fiasco” and are desperately trying to dig themselves out of losing every bit of scientific credibility.
Whether Brown is correct that the whole panic truly does trace to a brain flakeout on the part of Fauci – or even perhaps a deliberate “noble lie” to deceive the public into accepting the unacceptable – it hardly matters. The problem we face now is a huge tangle over terminology such that “infections” that could include as many as 90% false positives (according to the NYT) are called cases, while the once-distinct condition called cases which used to indicate actually being sick no longer has any precise meaning. The cacophony of statistical confusion here truly boggles the mind.
In the midst of all of this, the CDC itself finally updated its own estimates of the infection fatality rate of Covid-19. The CDC wisely took account of the huge demographic stratification of severe outcomes. There is not one rate that applies to the whole population or to any particular individual. There are only backward looking estimates of outcomes. They are all follows:
-
0.003% for 0-19 years
-
0.02% for 20-49 years
-
0.5% for 50-69 years
-
5.4% for 70+ years
Flipping the data to state it by survival rate by age:
-
99.997% for 0-19 years
-
99.98% for 20-49 years
-
99.5% for 50-69 years
-
94.6% for 70+ years
John Ioannidis sums up the disparity by age with the following infection fatality rate for people under the age of 70: 0.05%. This conclusion has been peer-reviewed and published by the World Health Organization.
How does this compare with the flu? We do not really know. As science journalist Shin Jie Yong has written, “There seems to be no data on age-specific IFR of the seasonal flu.” What this means is that crucial testimony of Fauci from March 11, in which he casually predicted based on bad numbers, that Covid would be ten times worse than the flu, can neither be confirmed or denied based on age-specific severe outcomes.
However, we can assemble the data based on years of lost life. Consider the long-term view over the future course of existing lifetimes. JusttheFacts reports:
If 500,000 Covid-19 deaths ultimately [in the future] occur in the United States—or more than twice the level of a prominent projection—the disease will rob about 6.8 million years of life from all Americans who were alive at the outset of 2020.
In contrast:
* the flu will rob them of about 35 million years.
* suicides will rob them of 132 million years.
* accidents will rob them of 409 million years.

As testing has expanded dramatically throughout the population, the estimated infection fatality rate of Covid will fall further. Thus can we observe a chart of “cases” (actually positive tests) all over the world and compare it with severe outcomes and see something remarkable that should make every living person fundamentally question why they decided to shut down the world and wreck billions of lives.
Another statistic that bears repeating, Covid – based on infections vs deaths – has close to a 99.9% survival rate. Imagine how the world would have been different had Fauci told that to the Congress on that fateful day of March 11. Or what if Fauci had revealed that the average age of death from Covid would almost equal the average lifespan in the US and exceed it in most parts of the world? People present might have wondered why they were holding hearings at all.
All these categories of data placement carry with them the danger of creating an illusion of control. Viruses do not come with little gears inside them with these rates. Human beings collect data and create them, and not one of them (whether IFR, CFR, infection rates, mortality rates, survival rates) pertains infallibly to any single individual. Our response to a virus is contingent on our own health, age, cross immunities, T cell memory, and a thousand other factors that no politician controls.
What we know is that a terminological confusion, a misplaced decimal point, a one-word error in data description, and a massive amount of arrogant presumptions about how to control a virus set in motion a series of events that turned our great and prosperous country into a disaster of confusion, demoralization, foregone medical services, closed businesses, wrecked arts and education, and long bread lines. The lockdowners who created this appalling disaster, the people who turned our trust into betrayal and a blizzard of statistical baloney, need to look at the science and data as they stand and come clean.
![]()
Zero Hedge’s mission is to widen the scope of financial, economic and political information available to the professional investing public, to skeptically examine and, where necessary, attack the flaccid institution that financial journalism has become, to liberate oppressed knowledge, to provide analysis uninhibited by political constraint and to facilitate information’s unending quest for freedom. Visit https://www.zerohedge.com